1. Do you have a balanced spine?
The vertebral column, also called backbone, spinal column is structurally balanced in front & side view to maintain the optimum flexibility to support the body weight. There are 3 gentle curves (cervical, Thoracic & Lumbar) can be seen in side view and in front the spine maintains the straight alignment.
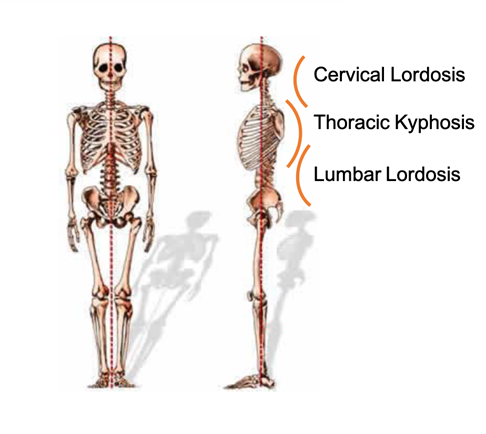
The body’s Center of Gravity (COG) lies around the level of naval and all of the spine’s flexibility helps to maintain this COG within the Base of Support (BOS) to stabilize the body during various activities. Maintenance of correct alignment helps to reduce the work load of the spinal muscles and fatigue during different activities (1) (2).
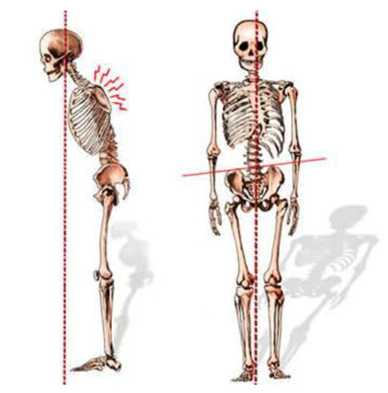
As displayed in the picture above, there can be sagittal (side view) & coronal (front view) spinal deformities occur in the human spine due to various reasons. When there is a deformed spine, the body posture & position of the COG changes. Therefore, to stabilize the body with these changes the muscles and the joints of the body required to work hard with an extra effort.
What is a bent spine (scoliosis)?
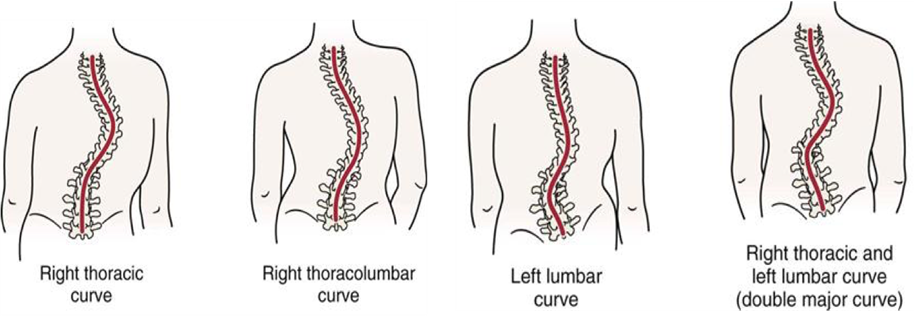
When there is a frontal misalignment in the spine, the spine will present with a lateral curvature of the spine more than 10° to the left or right with vertebral rotation. This spinal condition is called scoliosis (1). This is the most common abnormal curvature occurs in the spine, also considered as a world health problem and its prevalence is 0.5% to 3% of the world’s school population (3). On a x-ray of a scoliotic spine you will be able to see the presentation “C” or “S” shaped spine instead a straight one. Mostly the 80% of scoliotic curves are belonged “Idiopathic Scoliosis” category because it cannot be explained under a particular reason.
Scoliosis in Singapore
According to the University Spine Center at National University Hospital in Singapore, the incidence of scoliosis is 2.3%. This center sees 4500 to 5000 cases of scoliosis yearly and it is 7 times more girls than boys (4).
How do you check for scoliosis?
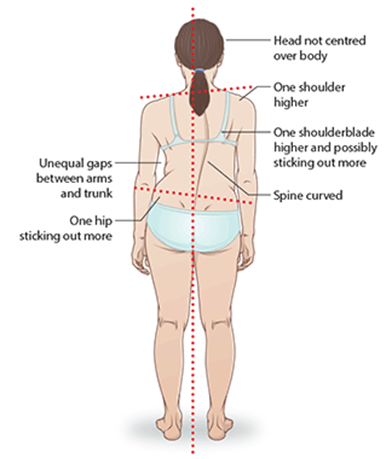
Scoliosis displays typical range of physical characteristics which also called clinical presentations or physical compensations. These clinical presentations are used to perform physical examination to assess and differentiate the bent spine (Scoliotic spine) from a normal one. Scoliosis research society guidelines says,
- When you stand in a relaxed position with your hands by the sides of your body; the back view may present with lateral (side) curvature, uneven shoulder blades and the shoulder, uneven hips and shift of the trunk.
- When you bend forward from the hips, a hump and a flank may see at the back.
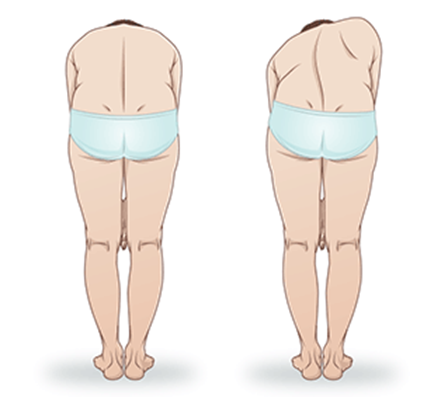
If you notice that you have these presentations you should consult a professional that can refer you for further examinations (5).
How can you confirm it is scoliosis?
When you consult a professional you will be guided through few examinations to ensure your spinal condition accurately.
- You will be directed to a spinal X-ray in sagittal (side) & coronal (front) views to confirm the curvature and it is wise to take a full spine X-ray from neck to pelvis.

- After examining the X-rays, the consultant will provide you the information regarding;
- Magnitude of the curvature (Cobb measure)
- Laterality of the curve
- Curve pattern
- Bone maturity
What are the treatment options available?
There is lot of debate regarding when & how to treat Idiopathic Scoliosis (IS) in the world. The American Association for Orthopaedic Surgeons (6) says “A scoliosis curve will not get straighten up by it -self” and “Spinal Braces or Spinal Fusion with Physiotherapy are essential in scoliotic curve management”. The Scoliosis Research Society (SRS) (5) has gathered information & evidences around the world and have suggested ideal treatments along with the factors that should be considered treating ‘IS’ patients.
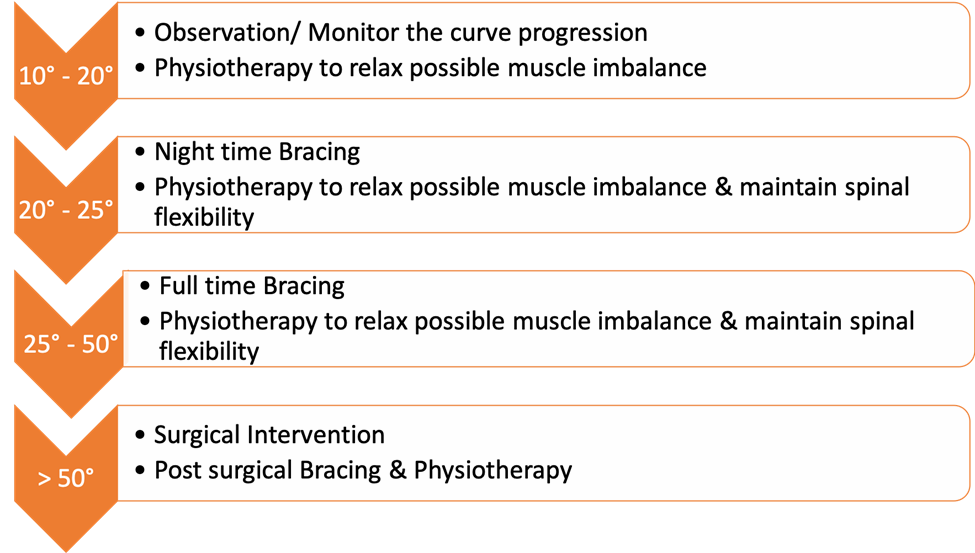
We have summarized SRS treatment recommendations for your easy understanding in the above picture. Any treatment for ‘IS’ should be re-evaluated in every 6 months with X-rays. Though there are certain negative effects with frequent exposure to X-rays these are necessary in observing the ‘IS’ curve progression (6).
As you can see, above treatment options are suggested mainly considering the curve magnitude as the base. But there are other factors also taken into consideration when prescribing above treatment options.
Key factors to consider when choosing your course of action
Age, Bone maturity, Menarche, Peak Growth Age and Curve Pattern are the other main factors that consider in choosing the ideal treatment option for the patients with ‘IS’ (7). Simple explanation below describes how does each of these factors can influence the ‘IS’ treatment protocol.
- Age – There are 2 periods of rapid growth spurts occur in life; one in infantile years and the other is in adolescent years. The height of the individual is increasing very fast during this time about 9cm per year. Also, the second highest spinal height increasement occur in 10 yo until puberty (7; 8). During this period, the curve progression is faster and it is best for you to keep in track with your age because there is a high probability to start bracing earlier for your curve instead monitoring. This is the golden window for spinal bracing.
http://helid.digicollection.org/en/d/Jh0211e/8.1.4.html
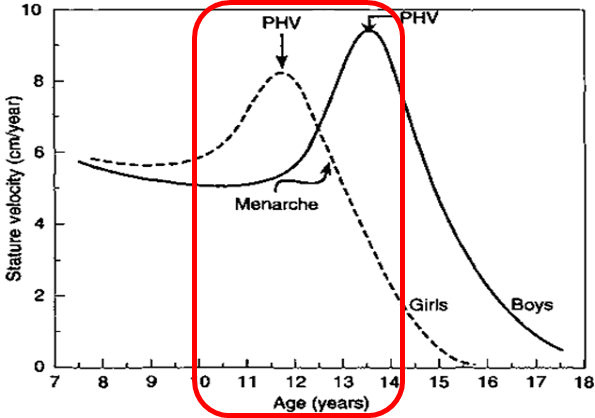
- Peak Growth Age (PGA) – This is the period both girls and boys show peak height velocity (PHV). It is very important to identify scoliosis patients before PGA, because there is a strong correlation with scoliosis curve progression with PGA. The parents who lost the opportunity to identify ‘IS’ at the age of 10 until puberty seizing this period for bracing is the 2nd golden passage to prevent massive increasement in the scoliotic curve (7).
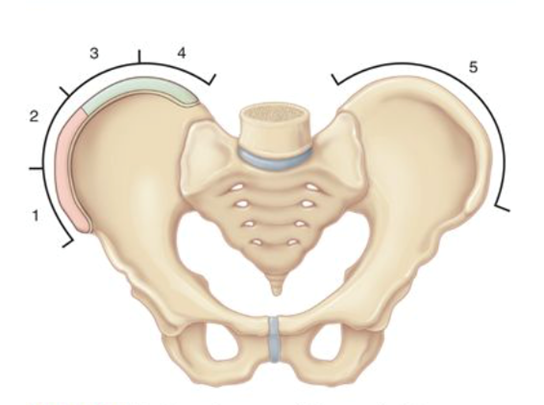
- Bone Maturity – The amount of growth remaining is typically estimated by Risser sign indicator. Risser Sign is a bony marker based on the iliac crest ossification. It ranges from 0-5; 0 indicating immature bone profile and 5 for matured bone profile. Immature bones are yet to grow thus worsens the scoliosis as the bones in the spine grow tall and fat (7). Therefore, a Risser sign of 0-3 informs that the curve progression is faster and early bracing is required to prevent further development of the curve.
- Menarche – In girls the onset of menstruation and in boys adult voice are indicators show the signs of slowing down the growth rate as the curve progression. Therefore, the requirement of the treatment mainly will be based on the magnitude of the curve as mentioned in the SRS guidelines. In this case parents and the school nurses should be responsible and attentive to screen out for any curve development in the spine after reaching the mature body state (7).
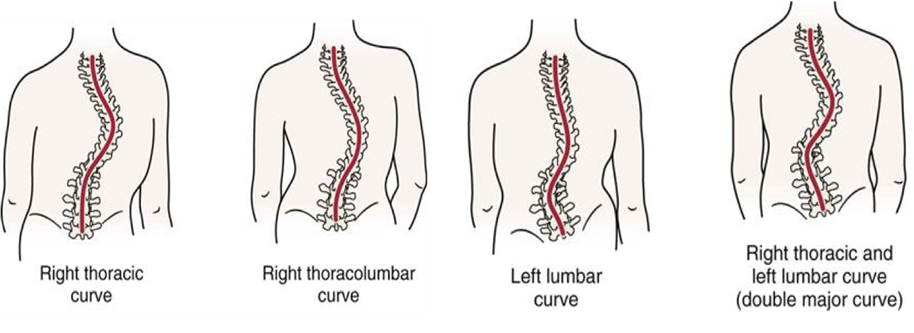
- Curve Pattern – Evaluation of patient history reports that the curve pattern also has a direct relationship with curve progression. Many researchers agreed on that single lumbar and single Thoracolumbar curves are less progressive and more responsive to orthotic treatment. Also, Single Thoracic curves and Double curves are more likely to progress faster (7).
What if I left the curve untreated?
Spinal bracing helps to stabilize the scoliotic curve, prevent further progression and often reduces the curve magnitude. Untreated scoliosis is progressive even after reaching skeletal maturity but the curves maintained less than 30 degrees with treatment aren’t progressive.
Patients with Thoracic curves and curve magnitude of 50-75 or higher experienced breathing difficulties, chronic back pain and cosmetic concerns related to age.
It is also very important to identify any presentation of scoliosis in early stages of the life between 1-2 years old and reappeared in adolescent years.
If untreated immediately these curves can progress very fast until 70 or higher degree within least amount of time. This can be further progress with the adolescent growth spurt.
If you missed the timing for the primary treatments and left with larger curves exceeding 50 degrees with mature bones you will have to seek for surgical interventions to prevent progression of the curves (7).
The ideal treatment protocol for bracing
Why Orthopaedia?
There are many types of spinal orthoses around the world are used to treat scoliosis. But we only use the best scientifically proven brace among all.
- 100% of our braces are manufactured & imported from Germany
- 100% of them are EU approved, quality-controlled braces
- 100% of braces uses body scans and CADCAM technology to design & modify the brace which enhance the accuracy of the corrective and de-rotational forces application on a 3-diamentinal setting.
- 100% clinically certified orthotists will be attending to your services
- Our treatment protocol is 100% similar to the Ideal protocol suggested by SRS.
- We use newest, scientifically proven, most effective technologies available in the world to treat our scoliosis patients.
The Orthopaedia Experience
Below we have attempted to simplify the mechanisms used in bracing at Orthopaedia for you to understand better why we only recommend the most effective option for our families.
Full Time Bracing – RC / RSC Brace
http://mayalassiter.com/2016/03/you-can-be-too-flexible-treating-scoliosis-with-a-rigo-cheneau-brace-schroth-and-postural-restoration/
https://scoliosisjournal.biomedcentral.com/articles/10.1186/s13013-017-0114-2
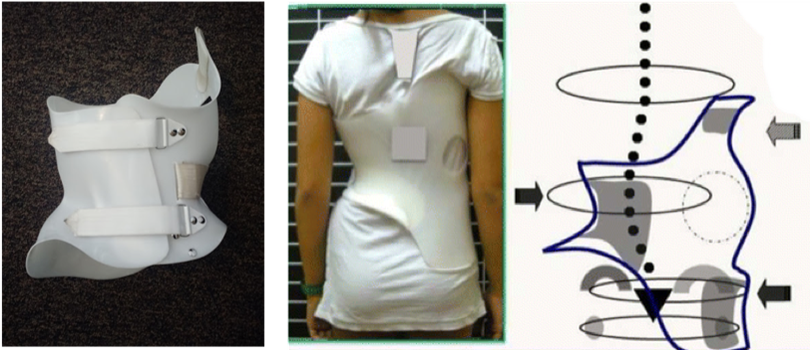
Rigo-Cheneau is a fully customized brace which applies over-corrective and ante-torsional forces to the scoliotic curves in the spine. As the scoliosis is a 3D condition RC brace also apply 3D correction to the trunk and the spine. This is an asymmetrical brace uniquely constructed with aggressive overcorrective and derotational forces with the expansions for trunk and spine to grow into best possible & morphological alignment. Scoliosis patients with higher rotational component in the curve are recommend to use RC brace as the brace designed with a primary correction for the torsion in the scoliotic spine (11).
Works Cited
1. Yenukoti, Rohith. CLINICAL ANATOMY OF VERTEBRAL COLUMN. https://www.researchgate.net. [Online] August 2015. https://www.researchgate.net/publication/328163417_CLINICAL_ANATOMY_OF_VERTEBRAL_COLUMN.
2. Oguz Aslan Ozen MD PhD, Ahmet Songur MD PhD. Spinal Anatomy. [book auth.] Christopher M. Bono Alexander R. Vaccaro. Minimally Invasive Procedures In Spine Surgery. NewYork : Informa Healthcare Inc., 2007.
3. Prevalence of scoliosis among school students in a town in southern Brazil. Lenice Sberse NeryI, Ricardo HalpernII, Paulo César NeryIII, Karin Passos NehmeIV, Aírton Tetelbom SteinV. 2, Brazil : Sao Paulo Medical Journal, Universidade Luterana do Brasil (Ulbra), 2010, Vol. 128.
4. Tai, Janice. SGH sees more cases of scoliosis with greater awareness. The Stright Times. [Online] November 11, 2018. [Cited: March 9, 2020.] https://www.straitstimes.com/singapore/health/sgh-sees-more-cases-of-scoliosis-with-greater-awareness.
5. Scoeity, Scoliosis Research. Conditions & Treatments: For Parents: Scoliosis. https://www.srs.org. [Online] Scoliosis Research Scoeity, 2020. [Cited: March 9, 2020.] https://www.srs.org/patients-and-families/conditions-and-treatments/parents/scoliosis.
6. Surgeons, American Association for Orthopaedic. OrthoInfor. Nonsurgical Treatment Options for Scoliosis. [Online] 1995-2020. https://orthoinfo.aaos.org/en/treatment/nonsurgical-treatment-options-for-scoliosis/.
7. Weibin Shi, Amy Strouse, Davis R Gater Jr. Orthoses for Spinal Deformities. [book auth.] American Association of Orthopeadic surgeons. Atlas of Orthoses and Assistive Devices. Philadelphia : Mosby Elsevier, 2019, Vol. 65.
8. Physiology of Growth. Rosenbloom, Arlan L. Basel : Nestec Ltd, 2007, Vol. 65.
9. Nighttimme bracing with the Providence brace in Adolesecnt Girls with Idiopathic Scoliosis. Charles Roland d’Amato (MD) (FRCS[C]), Sean Griggs(MD), Barry McCoy (CPO). USA : Lippincott Williams & Wilkins , 2001, Vol. 26. 18.
10. Irvine, Dr Paul. Treating Scoliosis without surgery. UK Scoliosis Clinic. [Online] UK Scoliosis Clinic, August 11, 2018. [Cited: April 14, 2020.] https://scoliosisclinic.co.uk/blog/why-choose-scolibrace/.
11. Brace Technology Thematic Series; The 3D Rigo-Cheneau type Brace. Manual Rigo, Mina Jelacic. 10, Barcelona : The Creative Commons Attribution, 2017, Vol. 12.